Medical Case Report
“C.M.” is a 32-year-old English single man, who does not suffer from chronic diseases. He works as a marine captain for one of the largest European companies specialized in ivory trade. He returned some time ago from the Congo after spending several months in the heart of the African continent.
His companion brought him to the emergency room for fear that he would suffer a sudden panic attack, as he was not in a stable health condition.
(The patient is unreliable in his account of events.)
- Patient complaint:
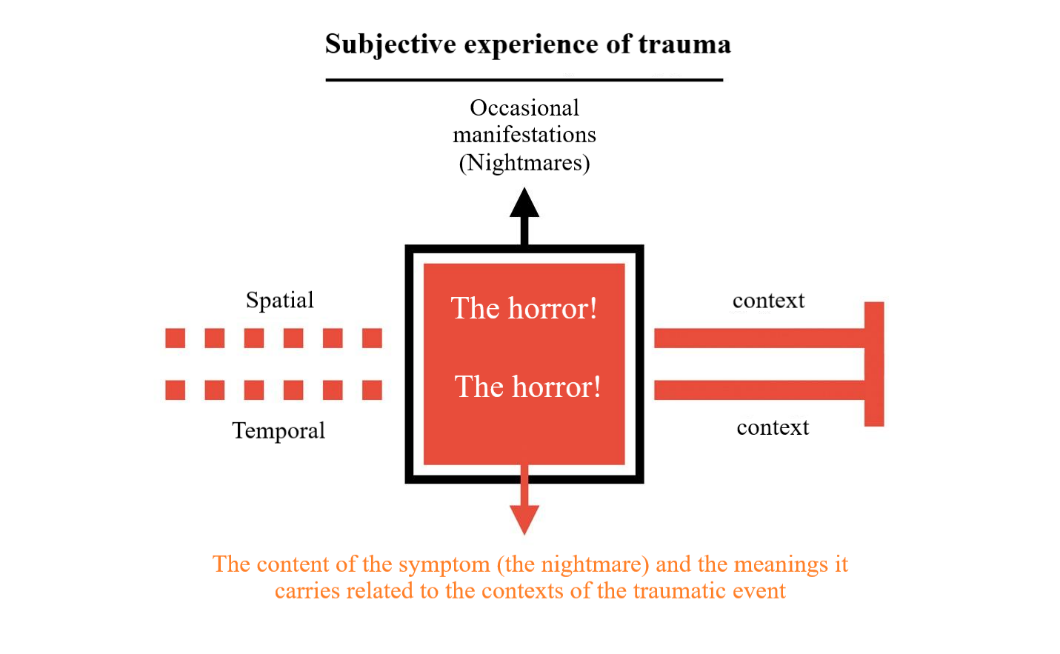
“I can still hear his voice ringing in my ears: “The horror! The horror!””.
- Detailed history of complaint:
C.M. was in a stable health condition before he went on a business trip to the Congo, where he sailed along the river that extends for thousands of kilometers for several difficult weeks, during which he was exposed to a series of tragic events that led to a significant deterioration of his condition. He told of the brutal scenes and corruption he witnessed, and of the greed of the company’s agents to plunder the land and its inhabitants. He also narrated his meeting with the so-called “Kurtz”, the legend of the ivory trade, and the dissident agent from the company, who set himself up as a divine figure among the tribes of the region in which he settled inside the Congo. We find him speaking with annoyance bordering on suspicion as he details Kurtz’s moral atrocities and his deadly quest for power. As he continued to narrate the details of the story, the patient mentioned that he was next to this mysterious man during his dying moments, when he heard him whispering: “The horror! The horror!” before he took his last breath. From that moment on, he felt the ghosts of this horror occupying his memory and controlling his thinking, and darkness began to haunt him wherever he traveled in the morning and evening.
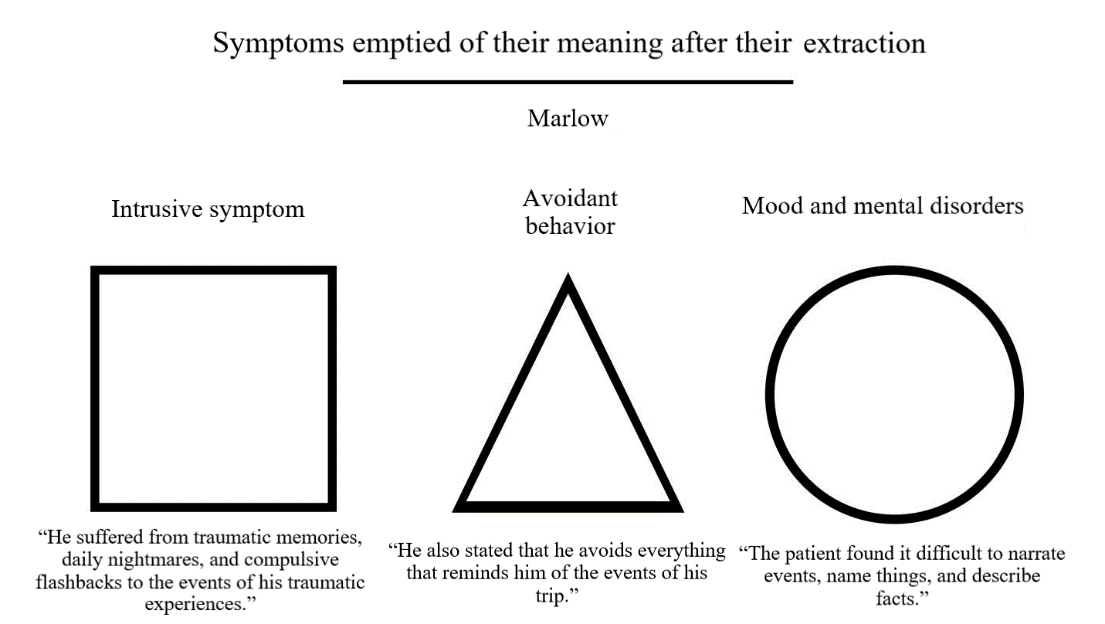
The patient was suffering from several recurrent intrusive symptoms, such as painful memories that impose their presence in his consciousness, daily nightmares about the atrocities he witnessed in the Congo, and compulsive recall of the events of his traumatic experiences and the physical and psychological upheavals they caused).
He also mentioned that he avoids everything that reminds him of the events of his trip, such as the company, ivory, and the memory of Kurtz and his terrible sayings that reflect the greedy nature of the human soul.
When asked about the details of his traumatic experiences, he found it difficult to narrate events, name things, and describe facts. He showed mood swings when talking about Kurtz’s thoughts and actions, and he also revealed his negative beliefs about himself, others, and all of European civilization.
Along with everything mentioned above, he was suffering from powerful dissociative symptoms, such as derealization and depersonalization, according to his description and the confirmation of those with him.
He denied any attempts – or thoughts – to harm himself or others or use drugs or drink alcohol.
- History of previous psychiatric illnesses:
Nothing noteworthy.
- History of previous medical illnesses:
Nothing noteworthy.
- Mental status examination:
CM looked pale and thin, despite his acceptable appearance in terms of cleanliness and grooming. His behavior was extremely suspicious, which was reflected in his speech that was characterized by confusion and misery. He was aware of his surroundings and deteriorating health (but he did not believe there was a treatment that could help him). His thinking was governed by despair regarding human nature and civilization, which made his behavior inappropriate in some situations, such as laughing in people’s faces. Although he denied auditory hallucinations, he would ask: “Don’t you hear it? The darkness is whispering urgently around us, a whisper that seemed to grow menacingly like the first breath of an oncoming wind: The horror! The horror!”.
- Diagnosis:
Post-traumatic stress disorder (PTSD) with dissociative symptoms*.
- Treatment plan:
In the case of an emergency, the patient was given (…), to help stabilize his condition,
Then he was prescribed (…), for a period of 14 days, and an appointment was booked for him to visit the clinic after completing the prescribed doses. He was also referred to a psychologist to schedule his treatment sessions*.
- End of report:
It may occur to some people that C.M.’s case and his story seem familiar in its details, and this is true. He is considered one of the most famous fictional characters in the history of fictional literature. If you have ever read Joseph Conrad’s novel Heart of Darkness (or watched Francis Ford Coppola’s film Apocalypse Now), you will recognize this character who has captivated the minds and imaginations of readers for more than a hundred years. He is Charles Marlow, the main character of this immortal story.
But what is the relationship between psychiatry and literary stories? To answer the question, we must first consider the style of writing the medical report, then consider the ability of the style to depict Marlow’s psychological suffering. Did the report succeed in depicting “The horror!”, as Conrad did in his novel? Simply put, no. And in fact, that’s okay. No one demands that doctors become writers like Dostoyevsky, Kafka, and Conrad himself when writing their patients’ reports. But there is something disturbing that cannot be overlooked in this sensitive issue, something related to our stories in our real world. What about our suffering, fears, and trauma? How does psychiatry deal with the stories we tell about “The horror!” in our lives?
The story of “C.M.” is not real, but the writing style that summarized his blatant suffering, as we saw in his imagined report, is the same style that will reduce the suffering of patients in their dealings with the psychiatric institution.
Lost meanings and scattered souls
With the identity of “Charles Marlow” being revealed, we will find ourselves facing an urgent problem that forces us to stop and look at what was written in his medical report, a problem that we can pose in the following question: Why did the report ignore Marlow’s narrative, and then reduce his suffering to vague descriptions, such as: “difficult weeks,” “traumatizing events,” “traumatic experiences,” etc.? By narrative here we do not mean the sequence of events, but rather the value that the events themselves carry. Because storytelling, as a narrative act, does not only mention the events of a story, but also attempts to frame it in an effort to contain and understand its meaning. That is, ignoring Marlow’s narrative in his medical report (as his words do not exist except in very rare cases) led to the denial of any possibility of comprehending the meaning of “The horror!”, which constitutes his greatest concern. This is because the central value of meaning from the perspective of the individual’s experience is carried in the context of his lived life in its cohesive, panoramic form.
We live within spatial and temporal contexts from which we cannot escape, as our embodied existence places us in a specific geographical spot and a specific historical point, what makes us perceive the world around us on the basis of the interactive nature between our “senses” inherent in ourselves, and the “environment” imposed by the context of our lives. Accordingly, we say that environmental factors play a fundamental role in shaping our cognitive frameworks and the values they carry for us that draw the features of reality and color it.
In the case of Marlow, we see his cognitive framework formed based on Victorian values in England in the late nineteenth century. He believes in the superiority of European civilization and its enlightenment project. From this framework (as Marlow perceives the world), we say that what he witnessed in the Congo is not merely “moral atrocities” as the report describes, but rather “crimes of imperialism under the rule of King Leopold II.” There is a difference that cannot be ignored between the two sentences. The first takes a brief, decontextualized snapshot, while the second paints for us a panoramic picture of the contexts that carry the meaning of the event.
The importance of this holistic view is that it is consistent with the often-misunderstood nature of traumatic experiences. The impact of psychological trauma is not limited to the brain and its functions, but also affects our experience of the world and our presence in it. That is, trauma from this perspective has a subjective dimension that we do not see in the objective writing of patient reports. It is trauma as a shattering of the cognitive framework, in which the values and meanings we carry in this world collapse, and our interaction with it becomes marked by the impact of our traumatic experiences.
Returning to Marlow, we see that it is unfair to reduce his suffering to pathological symptoms, such as nightmares, delusions, and others. Because this pushes us away from the essence of his shocking experience, which is his firm belief in the superiority of European civilization, and the nobility of what it does in countries like the Congo! Here, the nature of the shock that Marlow suffered throughout his journey is revealed to us. It is the shock of truth, the truth of imperialism, the truth of alleged superiority, and the truth of brutality that led to the commission of one of the largest massacres in human history. It is the shock that causes the collapse of everything he believes about the world; it is “The horror! The horror!” which has been haunting him since his return from the heart of darkness.
Now, it’s time to ask: What causes a psychiatrist to reduce the experience when dealing with patients’ complaints?
Tell me what’s bothering you… without telling me what’s bothering you
In a previous article entitled “The Doctor’s Missing Tool,” I mentioned that the doctor’s starting point in diagnosis is the objective characteristics of the complaint, not the complaint itself, with its subjective, incommensurable values. The experience of the patient’s suffering when he complains of a symptom is of a ghostly nature that cannot be captured objectively, which makes it difficult to describe, classify, and explain. Here comes the role of reductionism, which breaks down subjective experience into topics that can be medically diagnosed; for example, when the doctor reduces the diabetic patient’s experience (which affects most aspects of his life) to the numbers of his cumulative blood sugar results only.
But what about the experience of psychological suffering? Those for which there are no diagnostic tests and analyses? We do not examine an individual’s experience as we examine his body, nor do we measure mood disorders as we measure blood sugar levels. Here, it becomes clear to us that reductionism in psychiatry is of a different kind, a reductionism based on emptying experience of its subjective values, so that it is more amenable to objective description and classification.
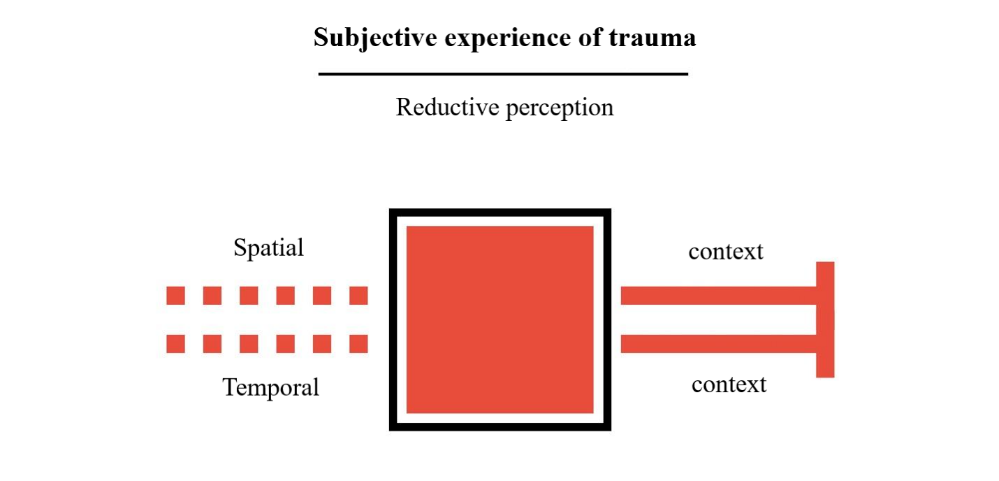
Let us return again to Marlow and imagine his subjective experience with the nightmares that began to haunt him after his return from the Congo. As we previously mentioned, this experience is rooted in the nature of his embodied existence as a son of the nineteenth-century European culture, and we cannot understand the meaning of “The horror!” that he complains about without placing his suffering in these spatial and temporal contexts.
In this illustration, the dilemma of psychiatry in dealing with the complaint of “The horror!” is revealed to us; it is imbued with subjective values and meanings that are inconsistent with the nature of medical practice. Medicine, as an objective science, is based only on firm foundations of general health phenomena that all humans share. How can we gather all the diverse subjective experiences of humans in their various cultures spanning the ages under one umbrella of psychological illness?
The traditional approach in psychiatry tells us that the solution lies in reducing experience for the purpose of describing and classifying it. That is, extracting all subjective values (with their cultural, historical, and social burdens, etc.) from the experience of psychological suffering, so that in the end we are left only with what we can easily deal with, such as the truncated symptoms that we saw in Marlow’s report.
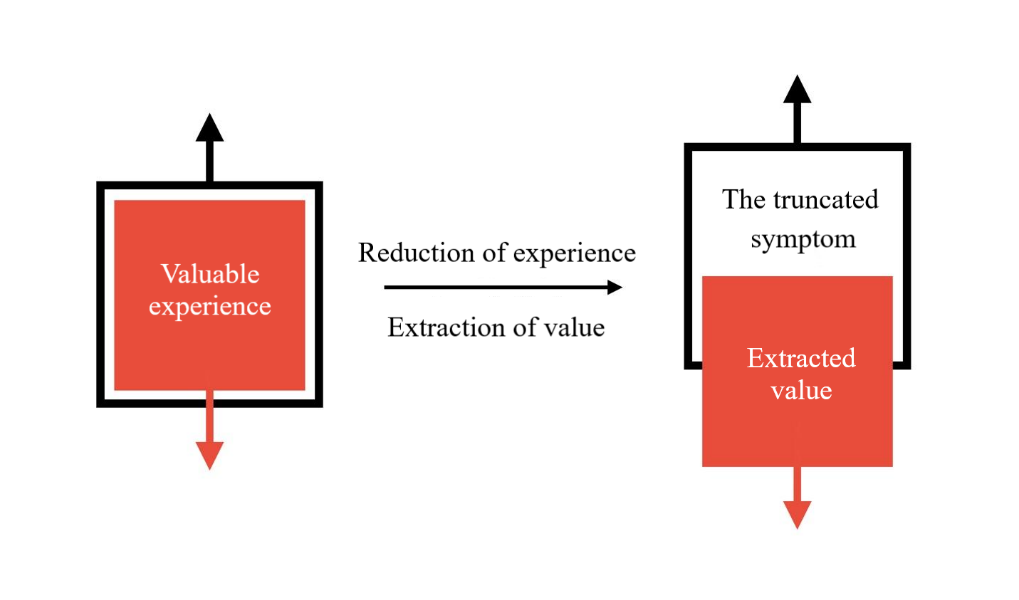
Now, let us imagine the same extraction process for all the symptoms that Marlow complains of.
Here, we come to what psychiatry claims is the established basis for psychological illnesses among humanity with their various experiences. It is the diagnostic criteria for the truncated symptoms that would define the case of Marlow, the young man who miraculously survived a fatal car accident, the young woman who was sexually assaulted, the soldier who fought bloody battles, and the mother who lost her son during birth, and the father who lost his fortune in a scam, under one umbrella called: Post-traumatic stress disorder (PTSD)*.
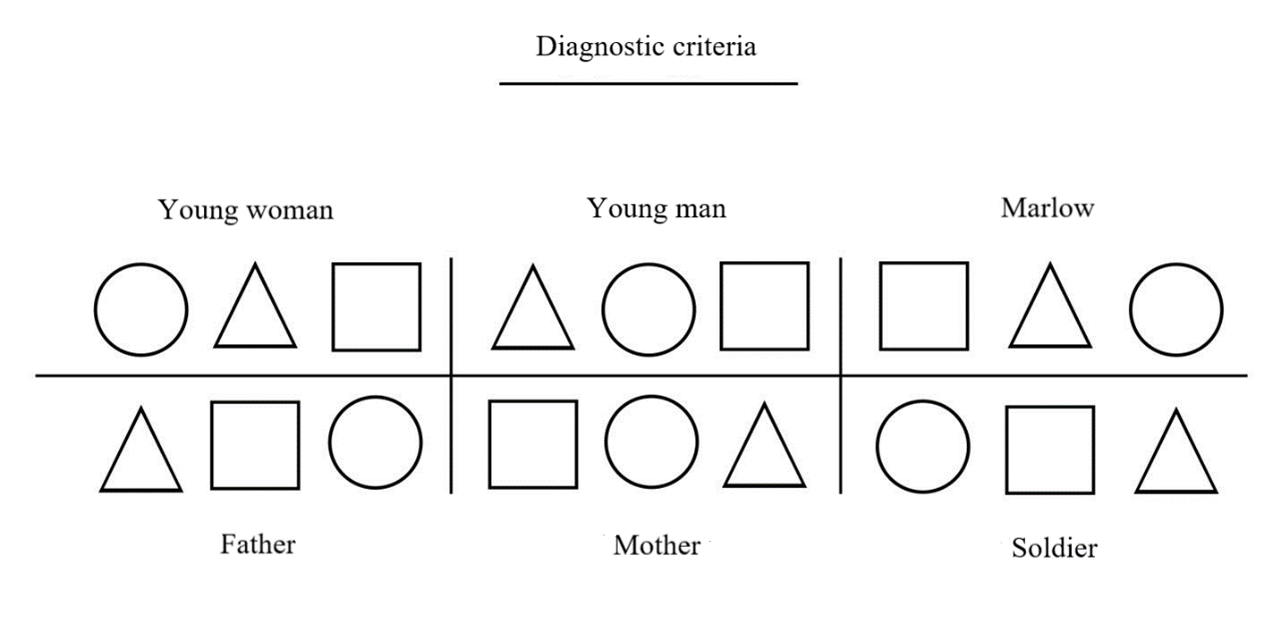
From a neutral position, we cannot criticize this trend in its entirety, as there are stacks of scientific papers that tell us about the tangible impact of trauma on our bodies and brains. But we have already emphasized the importance of the existential impact of trauma as well, that which is concerned with our experiences and perception of the world. All six may share the same disorders, behaviors, and symptoms; but they will not share the same experience! This is because the nature of the trauma from the car accident is not like sexual assault, nor is it like participating in war, nor is it like any other trauma. Seeing as each incident has its own experience that weaves meanings into the contexts of the victim’s lived life.
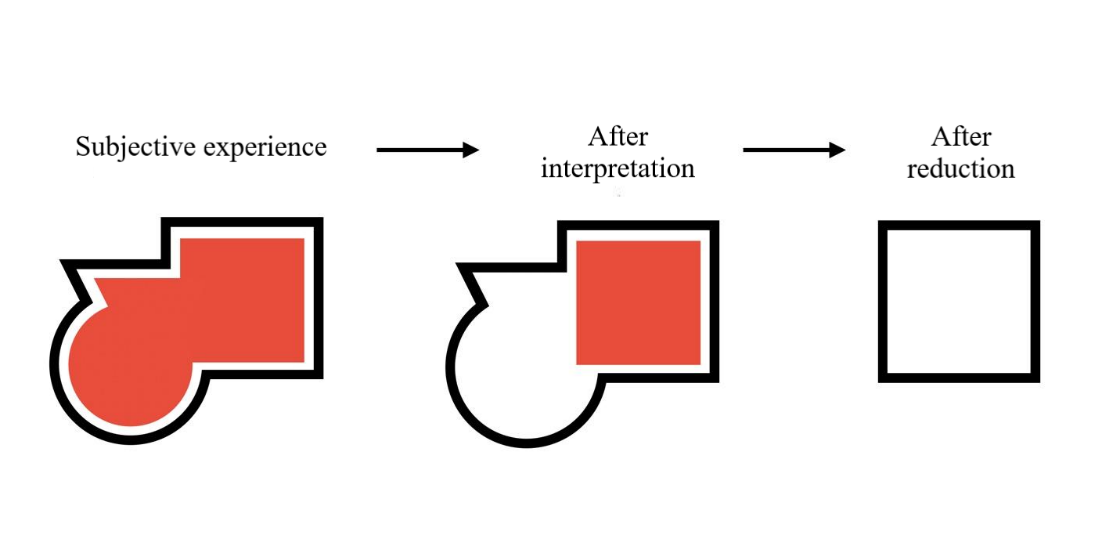
What we are calling for here is not to completely abandon diagnostic criteria, but rather to support them using the necessary philosophical tools, in order to ensure the integrity of the presence of subjective experience with all the values it carries when diagnosing and treating, and that the patient’s condition does not end up with symptoms truncated from their contexts, such as the empty geometric shapes in the illustrations.
But it seems that there is something unpalatable in this cognitive proposition, even when it is deconstructed and criticized. It seems as if psychiatry, with its reductionist orientation, has forced us to play according to its rules!
The biological narrative of psychiatry…a failed success story
We do not need a long review of personal experiences here to notice the problem in portraying our suffering in this simplified form. Our experiences are more profound in their reality, and our stories are more complex than what is written about them, so what prompts us to think in this reduced way? Let us now take a step back and reformulate our perceptions again. In order to do this optimally, we must first understand what we mean when we say that “psychiatry forced us to play by its rules.”
This newly discovered field has been plagued by a huge legacy of attempts to objectively study, analyze, and classify mental illness. We can say here, with some confidence, that the field of psychiatry is still struggling in its attempts to make real progress at the scientific level (especially with regard to providing adequate explanations for the diversity of subjective experiences among humans). But despite all these difficulties, its biological narrative was not affected by imposing its language, definitions, and ideas on all of us. Today, under its conceptual control, we define ourselves according to its interpretations, and classify our pain according to its criteria. We have begun to think from its reductionist principles of human nature, and repeat its speeches that we are nothing but robots governed by the activity of their brains.
Here comes the role of the philosophy of psychiatry to curb biological reductionism, and to remind science of the limitations of its tools when dealing with our diverse experiences. This is because our feelings, aspirations, and memories are not “natural phenomena” that can be placed in a laboratory, analyzed, and described. There is something in the nature of experience, in its intrinsic value, that is difficult to capture using current and even future scientific tools. Our experiences are a thread of the fabric of human experience spanning thousands of years (from the era of primitive drawings on cave walls… to the era of technical revolutions in the twenty-first century). We are not part of history, civilization, and society; rather, we are history, civilization, and society. This is something that cannot be reduced.
Therefore, we must be careful, even as we criticize psychiatric practices, not to fall victim to its reductionist language. We have to accept our complexities and take the difficult road to understanding ourselves and the world around us.
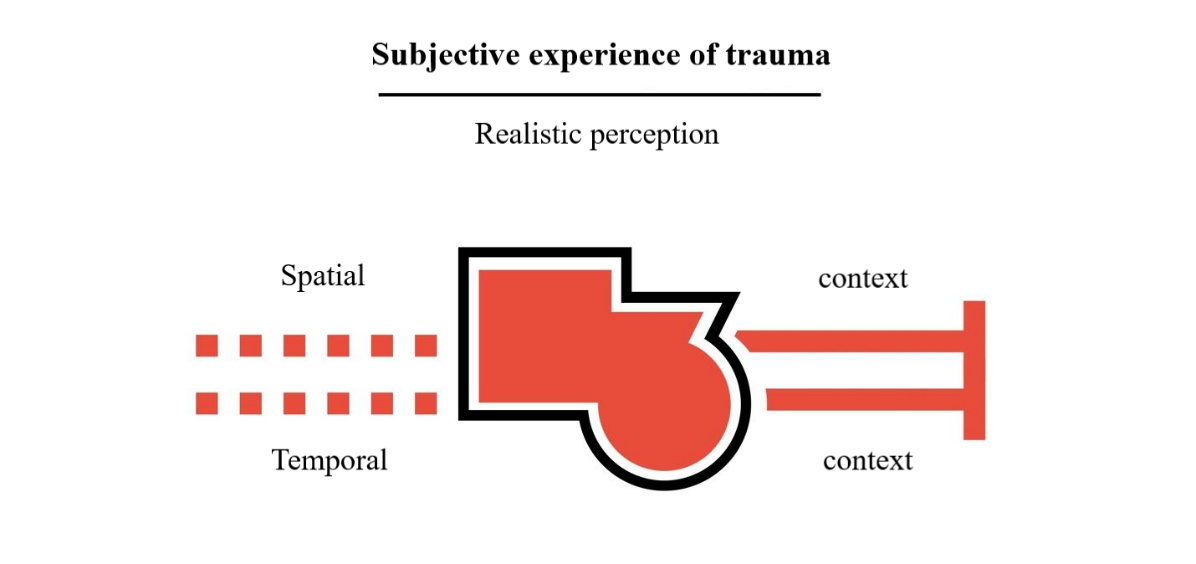
Squares, triangles, and circles do not exist in real life, which means that we have to retreat from this previous perception,
and replace it with a more realistic perception that is closer to the complex human nature.
This change in our perception of subjective experience will bring us back to the method of medical writing, to ask the most important question in this article: How will what the psychiatrist writes in the report affect the patient’s definition of themselves?
From “Charles Marlow” to “C.M.”, the making of the reduced self
Can we name this form in realistic perception? Simply put, no. This applies to our traumatic experiences as well; it inherently challenges language’s ability to name and delineate reality, making it difficult to know. Hence, it leaves the individual in a stage of intense vague feelings. Nothing expresses these feelings more than the saying: “The horror!” The horror!” It reflects the individual’s inability to grasp and name their traumatic experience. If the patients are unable to describe what they are suffering from, what makes the doctor confident in what he writes in the medical report?
The answer to this question is no less terrifying than the suffering of the patients themselves! Because psychiatric reports are not objective facts that describe the reality of the patient’s complaint, but rather the doctor’s interpretations of what this reality might be from his own perspective. That is, the psychiatrist who is only good at dealing with diagnostic criteria (simplified geometric shapes) will interpret complex subjective experiences to suit their available tools. This means that there will be several interpretations of one complaint.
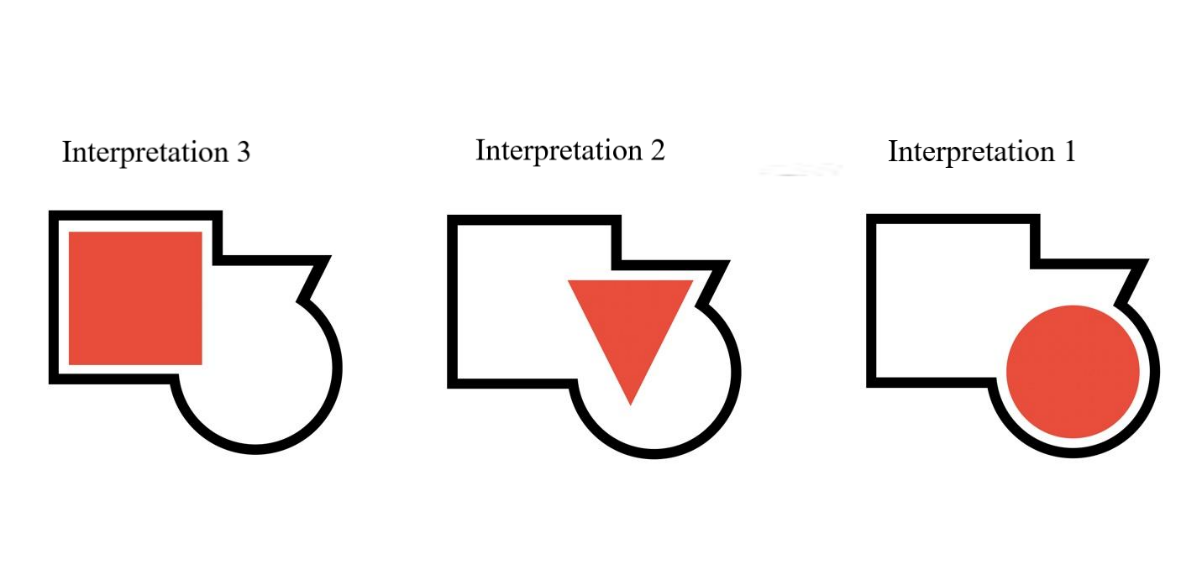
Here, medical practice takes an extremely sensitive, authoritarian turn, because what the psychiatrist does when writing the report is not a formulation of the complaint and its symptoms, but rather a formulation of the patient themself! That is, interpreting experience and then reducing it necessarily means creating a different self, emptied of values, abstracted of its humanity, which can be included in diagnostic criteria without problem.
What will happen next is that the patient will be thrust into a vortex of medical interpretations that will produce and reproduce the shortened narrative of his suffering. The doctor will write his own interpretation in the report as an absolute truth, ignoring the rest of the basic dimensions of experience and the contexts of living life. In this simplicity, the patient will find themself in the middle of a maze from which they cannot get out, because everyone who reads their medical report will be affected by what is written and will deal with them accordingly.
Indeed, the issue becomes more complicated when what is written in the report is considered the absolute truth of the complaint. In this case, the patient is locked into the diagnostic criteria during their successive visits with psychiatry. Because what is written in the reports of previous visits will affect the questions of future visits. This influence is often directed towards emphasizing the narrative of the medical team rather than the narrative of the patient themself. That is, the wording of the doctor’s question will come to extract a specific answer, and this answer will be recorded after being interpreted to fit what the doctors wrote previously.
If you are placed in a diagnosis box, you will face great difficulty trying to get out of it, because every doctor, after seeing your medical report, will try to put you back in it or put you in the next box. This may push you, in one way or another, to replace your own narrative and adopt the biological narrative. Here, the power of the psychiatric establishment is revealed to us, which not only marginalizes our narratives and stories as we live them, but also forces us to believe that we suffer because of some imbalance in our brains.
These writing practices, which center around the narrative of the strongest and marginalize the voices of the weak, are among the most prominent issues that literary criticism addresses when it tackles themes of power in narrative works. Can we use literature and its critical trends to understand this impasse and try to get out of it?
From the heart of darkness to the heart of the clinic
There are facts that cannot be overlooked when we talk about the novel Heart of Darkness, the most important of which from a critical perspective is Joseph Conrad’s marginalization of the African narrative when he depicted the atrocities of colonialism, and his focus on European points of view represented by Charles Marlow and Kurtz. Conrad placed the land and its people in the background of his moral questioning of the colonial project, without allowing them to speak about their stories and suffering! Edward Said says, criticizing the author of the novel: “Because he is a product of his time, Conrad could not grant the indigenous people their freedom, despite his strong criticism of the imperialism that enslaved them”. What Said means that Conrad is unable to imagine an alternative to the colonial situation, despite its horror, and this is because he does not see the peoples of African countries as capable of ruling themselves; he is for and against imperialism.
Let us now consider reporting practices from the same critical perspective. How does a physician exercise their written authority when dealing with patients’ narratives?
Looking at the doctors’ position on the medical situation in crisis under the weight of the biological narrative, we will find there is a great similarity with Conrad’s position on European colonialism. The psychiatrist is aware that there are many negative effects resulting from the reductionist tendency of the biological model, but unable to imagine an alternative model that enables patients to share their narratives without interpretation or reduction. The reason behind this is that the doctor is the product of their academic institution and cannot imagine what is outside its borders. That is, their inability does not necessarily mean that alternative models do not exist, but rather it is an indication of the weakness of their critical senses in reality.
Final words
At the conclusion of this article, we must face the bitter truth, which is that the objective language of science is not appropriate for telling our stories, which prompts doctors to marginalize these narratives by using their written authority. The importance of documenting patients’ stories lies in their interpretive authority that resists reducing their suffering to every doctor who reads their medical reports. We find the patient saying after documenting their narrative: “Listen to me, this is my story, this is my life,” which gives the report an indispensable dialogic character. This word may be what we want to achieve throughout the article: “dialogue,” meaning two equal voices, not one dominant voice and the other marginalized.
Let us remember that Joseph Conrad presented the world with the novel Heart of Darkness to reveal the horrors of European imperialism, but this did not protect him from the stigma of hidden racism. Because what matters in achieving justice is that you enable those with vulnerable voices to express their suffering.
Marginal note*
(We note that the example of post-traumatic stress disorder (PTSD) mentioned in the article is simplified for the purpose of illustrating ideas only and should not be taken as an attempt at medical education.)
References

T1703